



科室医生 查看全部

科普·直播义诊专区 查看全部
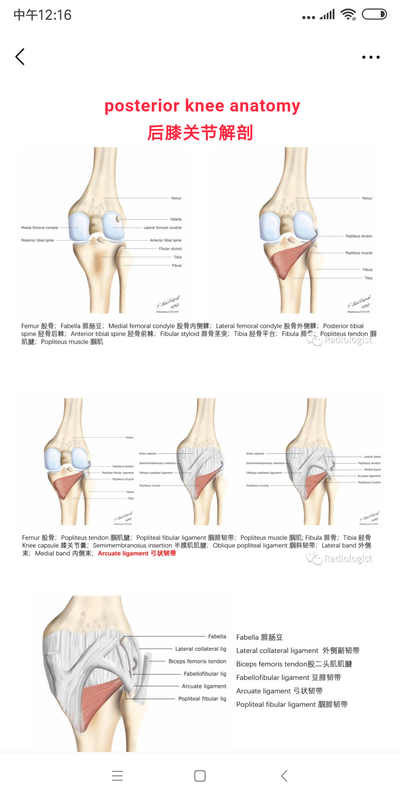
- 弓状征-膝关节弓状韧带损伤
The arcuate sign is often a subtle but important finding on knee x-rays and represents an avulsion fracture of the proximal fibula at the site of insertion of the arcuate ligament complex, and is usually associated with cruciate ligament injury (~90% of cases) . The fracture fragment is attached to the lateral (fibular) collateral ligament, the biceps femoris tendon, or both. 弓状征通常难以觉察,但在膝关节X线图像中这个征象非常重要,它代表了近端腓骨弓状韧带复合体附着处的撕脱骨折,这种情况常常合并交叉韧带的损伤。撕脱骨片系于腓侧副韧带、股二头肌肌腱或以上两者。 Clinical presentation(临床表现) The fracture results most often from a direct blow to the anteromedial tibia when the knee is extended, resulting in posterolateral subluxation of the tibia in external rotation . Alternatively, sudden hyperextension of the knee with the tibia internally rotated may cause the same injury . The importance of this injury is that if it is not diagnosed acutely, posterolateral instability may develop which is challenging to correct, and may result in failed cruciate ligament reconstruction. 导致这种骨折的原因通常是膝关节伸展时力直接作用于胫骨前内侧,结果胫骨外旋并向后外侧半脱位。另外,膝关节突然过度伸展时胫骨内旋可造成同样的损伤。 这种损伤的重要性在于,如果没有被及时诊断,可发展成膝关节后外侧不稳——一种极具治疗挑战性的疾病,并可能导致交叉韧带重建的失败。 Radiographic features(放射学特征) The shape and size of the avulsed fracture vary according to which ligaments are responsible. 撕脱骨折的形态及大小根据责任韧带的不同而不同。 Plain radiograph(平片) The avulsion fracture is usually small,
 李灿 医师 菏泽市立医院(总院) 放射科2454人已读
李灿 医师 菏泽市立医院(总院) 放射科2454人已读 - 骨巨细胞瘤的少见发病部位
骨巨细胞瘤(giant cell tumor ,简称GCT)为骨原发的良性侵袭性肿瘤,占原发骨肿瘤的20%,早期将其分在低度恶性中,后分为中间性(良恶性之间),现在的分类为良性侵袭性肿瘤(3期)。可以看出骨巨细胞瘤生物学行为复杂,多变。 骨巨细胞瘤病因不清。 年龄:20~40岁为最好发年龄,约占80%。 性别:无性别差异。 部位:好发部位为股骨下端和胫骨上端(膝关节周围),其次为肱骨近端和桡骨远端,其他部位有椎体、骶骨、髂骨、腓骨近端、胫骨远端等等。 症状:主要表现为局部疼痛,逐渐加重,随着病情进展,可有肿胀,压疼。如果发生骨折,则表现为突然剧痛、肿胀、畸形、不能活动。骨折诱因往往是轻微外伤。无发热、消瘦等全身表现。 辅助检查 1、影像学检查 X线平片:是最基本的检查,表现为骨端的溶骨性破坏,偏心,可有膨胀,无钙化和成骨。 CT:要做强化CT,可以看肿瘤的边界、范围,肿瘤的血运。 MRI:可以更好的显示肿瘤的边界,但不能代替CT。 ECT:骨巨细胞瘤个别情况有多发可能,全身骨扫描可以除外多发病灶。 胸部CT:骨巨细胞瘤有肺转移可能,需要做胸部CT。 疾病诊断 临床、影像、病理三结合。不要单一迷信某一项,尤其这三者有不符合时,要格外小心。 鉴别诊断 骨巨细胞瘤常常需要和以下疾病鉴别: 1、动脉瘤样骨囊肿:好发于青少年,往往合并其他肿瘤,如:骨巨细胞瘤合并动脉瘤样骨囊肿、软骨母细胞瘤合并动脉瘤样骨囊肿等等。单发动脉瘤样骨囊肿最好发部位是脊柱附件,位于肢体者影像学表现不易与骨巨细胞瘤鉴别。 2、骨肉瘤:好发于青少年,常见部位为长骨干骺端,病程短,症状重,影像学表现为长骨干骺端骨破坏,常有成骨,边界不清,有骨膜反应和软组织包块。病理表现为恶性肿瘤细胞直接成骨。 3、 骨囊肿:青少年好发,常位于肱骨近端和股骨近端,多以骨折为首发症状,X线表现为中心性、膨胀性改变,边界清楚,CT无强化。 下面介绍一例骨巨细胞瘤的少见发病部位的病例。 我们都知道骨肿瘤的发病部位对于鉴别诊断至关重要,今天分享一个常见骨肿瘤,但发病部位少见,不知您能否一看看穿! 18岁的男性,因手指疼痛就诊,以下是影像学资料。
 李灿 医师 菏泽市立医院(总院) 放射科1685人已读
李灿 医师 菏泽市立医院(总院) 放射科1685人已读 - 剥脱性骨软骨炎/骨软骨缺损
看到OCD,大多数肌骨方向的同仁表示耳熟能详,但确有不少人对其内涵及病理演变不甚了解,甚至有人忽略了病理基础和临床病史而出现诊断不精确的情况。 为了响应“精准医学,影像先行”的号召,今天我们对OCD进行一次刨根问底的分析。 OCD is an abbreviation which can stand for either Osteochondritis Dissecans or Osteochondral Defect. 我们来给OCD下个定义:OCD,既可以代表剥脱性骨软骨炎,也可以代表骨软骨缺损。 Osteochondritis dissecans is used when the patient is young and the cause is not exactly known, yet most probably due to repetitive microtrauma. 剥脱性骨软骨炎常用于下属情况的诊断:患者年轻,病因不明确,大多数情况是由于关节反复的轻微创伤。 Osteochondral defect is mainly used when a patient is older or when a particular trauma is thought to be the cause of the defect. 骨软骨缺损常用于下属情况的诊断:患者年龄较大,明确的创伤病史。 Both describe a joint defect which involves the articular cartilage and the underlying subchondral bone. 两者都用来描述关节结构的缺损,涉及关节软骨和软骨下骨。 When a small defect in the chondral plate is present, the intraarticular fluid will erode the subchondral bone, which will result in bone marrow edema. 当关节软骨出现小的缺损时,关节液就会侵蚀软骨下骨,进一步导致软骨下骨的骨髓水肿。 This process can evolve into cyst formation. 这种病理过程可进一步导致软骨下骨的囊性变。 Finally, when fluid flows underneath the defect, the OCD can become unstable and may result in a corpus liberum. 最终,关节液在缺损部位下方流动,OCD可以使受累骨不稳定,而形成关节游离体。 下面是三个病例,分别代表着OCD的不同病理阶段:软骨下骨髓水肿,囊性变,不稳定OCD及其下方积液。
 李灿 医师 菏泽市立医院(总院) 放射科2905人已读
李灿 医师 菏泽市立医院(总院) 放射科2905人已读
问诊记录 查看全部
- 冠心病 在菏泽市立医院拍了个冠脉ct,报告是前降支轻度狭窄,其他血管... 看一下片子总交流次数51已给处置建议
- 想咨询下面部核磁共振检查面部注射异物 半年前注射不明针剂,导致面部有增生,想做面部核磁共振检查一下... 想咨询下能否可以做面部核磁共振检查面部注射异物总交流次数2已给处置建议
- 患者:男 39岁 右膝股骨小片骨髓水肿 最后交流时间 2021.12.23右膝股骨小片骨髓水肿 右膝股骨外髁软骨损伤总交流次数47已给处置建议
- 这些没有啥症状,都正常 我上周一带孩子我闺女30个月3岁去做的脑ct、我想总交流次数13已给处置建议
- 咨询低剂量ct 你好,大夫,两个问题:一是请问咱们医院有低剂量ct总交流次数2已给处置建议